Design as an Agent for Change:
The Need for Collective Intelligence.
We see design as a profession whose aim is the improvement of the welfare of people. To achieve this, the very nature of the problems faced force us to work collaboratively. If one is going to do something important, it’s quite likely one is going to do it with others. Working with others becomes significant when everybody contributes to everything, from different points of view—something that designers, when working in teams, should lead others to do. The potential benefits of integrating the work of many at their best, with all their different perceptions, priorities, hierarchies, and levels of responsibility, could be defined as the capitalization of collective intelligence. This practice is not restricted to designers, but extends to clients and users because as designers we do not work for them; we work with them.
 Designing collaboratively is an act of partnership. This relationship implies synchronicity—having a common purpose and a common responsibility—as in a symphonic orchestra. It is during this process of communicating and working in partnership where people form bonds, and reach consensus. They do this interacting, conversing, listening, observing, learning and collaborating in an atmosphere of empathy and care for others. All of these interactions encourage people to become highly motivated, and able to give their best response to design problems.
Designing collaboratively is an act of partnership. This relationship implies synchronicity—having a common purpose and a common responsibility—as in a symphonic orchestra. It is during this process of communicating and working in partnership where people form bonds, and reach consensus. They do this interacting, conversing, listening, observing, learning and collaborating in an atmosphere of empathy and care for others. All of these interactions encourage people to become highly motivated, and able to give their best response to design problems.
In design as collective intelligence, designers seek advice to understand the issues and identify what is needed. They are active listeners, not only keeping quiet when listening, but rather identifying key issues, common interests, values, purposes, barriers and opportunities in the speech of the other. For design as collective intelligence to materialize, what is required?

Design as Collective Intelligence:
The Need for Good Leadership.
Leaders in design projects do not have to be appointed bosses; rather, all members of a working team can be leaders, using their capacities to help everybody else get the best out of themselves. Good leadership is distributed leadership; it is not top-down, it decentralizes decision-making processes, motivating instead of demanding, and empowering people without controlling them.
Design as collective intelligence requires flexibility to adapt to different problems, users, disciplines, situations and resources without diminishing the group’s capacity to deliver a top-level response. To look at design problems in different ways and to respond to constantly changing situations requires not only flexibility, but also mental and social agility in order to go beyond the ability to adapt to change, and instead generate change.
In addition to the dynamics of designing with others, designers also have to be aware of the inertia of systems and their resistance to change, and be agile and prepared to overcome that resistance.
Designers must know the systems within which their projects operate. Designers must be keen observers. Designers must also have good communication skills. Good communication skills foster the creation of a feedback rich environment.
In design as collective intelligence, people are resourceful, reacting properly in difficult or ambiguous situations; coherent and honest, so that they are understandable to others, and thus generate trust in their ethics, knowledge and judgment skills; courageous, to make difficult decisions when decisions are needed and doubt paralyses others; and self-aware, to know where the limits of their knowledge and abilities are, and when to seek advice.
Collective intelligence flourishes when people apply their disciplinary knowledge while interacting with others, offering fresh views on the topics at hand and engaging in mutual understanding processes. It must here be mentioned that interdisciplinary work requires disciplinary competence.
Very often, we can find ourselves working with controlling leaders or controlling clients; these people promote passivity, fear, and collective stupidity. To create the best possible design work, designers need good clients and good team members. But where did we learn that? Was it at school? Are we teaching this to our students? Let us now move to our experience as designers, and explore the kinds of situations in which we have worked.
How Do We Work?
At Frascara-Noël we practice a design that is user-centered, evidence-based and results-oriented. To do this, we use several tools and strategies including prototypes, iterative designing, empathic approaches, diagrams, problem-based learning, and interdisciplinary teams. To begin with, we include the users in our design process sooner or later, and preferably sooner. The users are the experts; our best allies when trying to understand our design problems are the people who suffer them, and for whom we have to create better situations. We use these tools to connect people, produce high functioning teams, collaborate on multiple scales, and encourage effective peer production.
Example One: The Blood Transfusion Form
In 2009, we redesigned a hospital form used to request blood components for transfusions in an Italian Hospital (Figure 1). Our users were directors of hospital facilities that normally need blood, such as Surgery, Gynecology and Hematology.
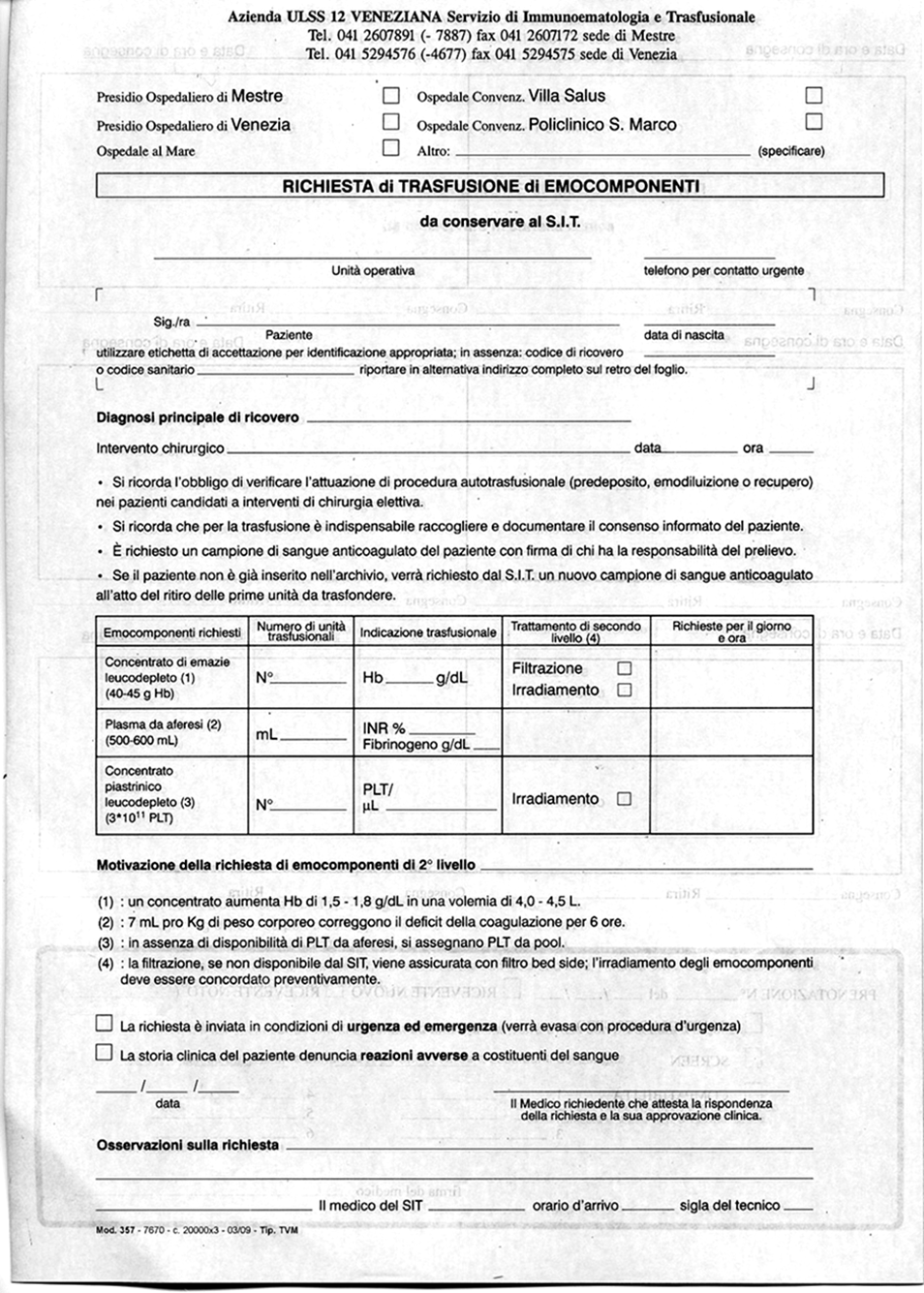
A form is a tool, an administrative tool, and it should help people perform their task easily and efficiently. Through observations and dialogue with users, we first identified how the form was used, what the obstacles to its use were, and what it was supposed to do. We then developed what we call performance specifications. We observed that in an emergency situation, for instance, when a gynecologist needed blood urgently, he did not fill out the form himself, but asked a nurse to do it. This practice, obviously, created an overload on the nurses’ part, and was detrimental to both the nurses and the overall efficiency of the hospital.
These issues suggested that the tool presented design difficulties that needed to be addressed. When the gynecologist was available to talk with us, he explained the barriers posed by the form. The main barrier was the time and cognitive effort filling it required, taking the doctor’s attention away from his main task of caring for the patient.
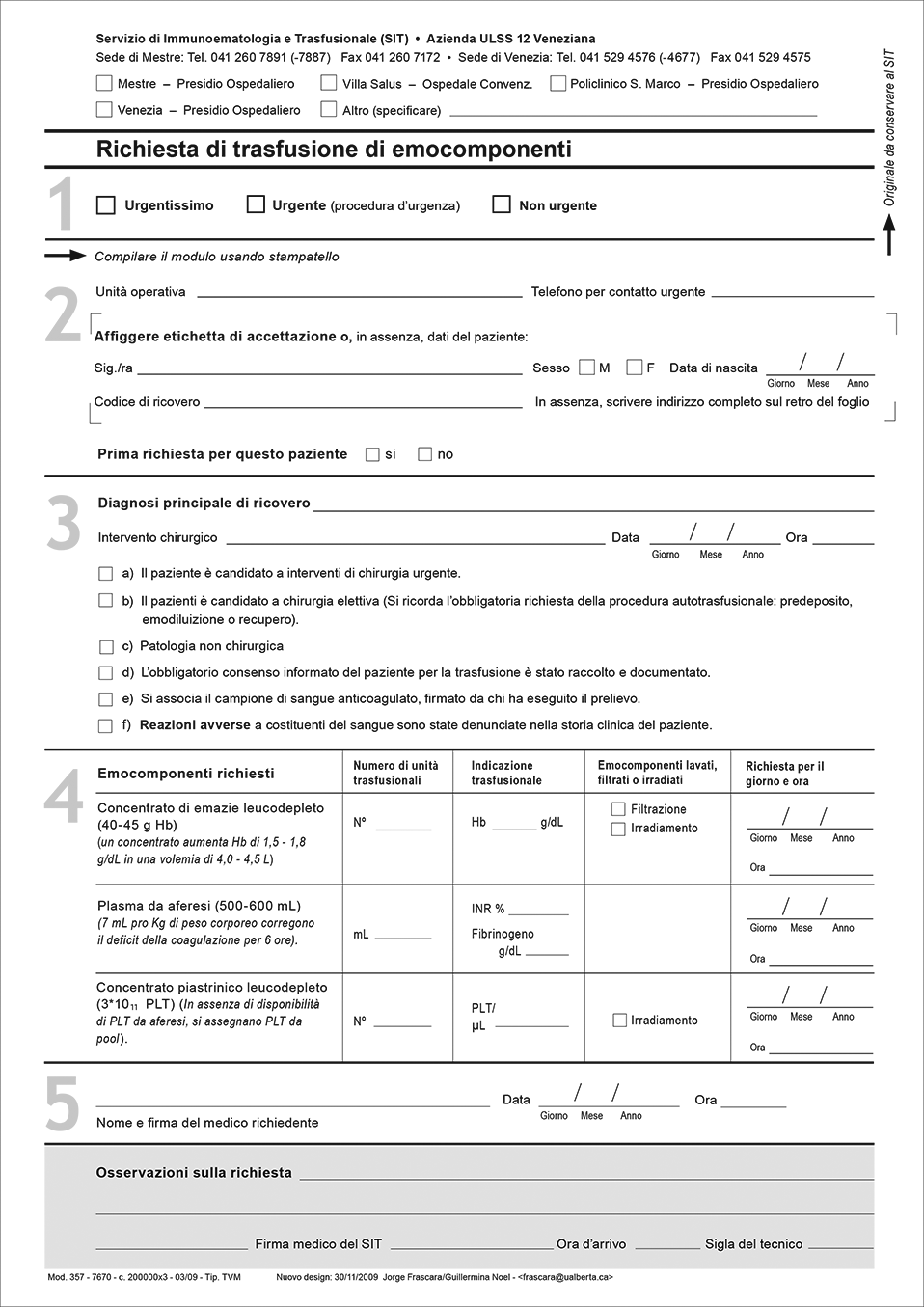
Through the design of prototypes, we started an iterative process of design and interviews. Eight prototypes were necessary to arrive at a solution that we could consider successful (Figure 2). Prototypes create common grounds that help us communicate with others, focus the conversation, and reduce possible misinterpretations. The prototypes we developed resulted in 52 modifications to the existing form. We got a good level of cooperation from the client and the users, particularly when a meeting was called to harmonize the different perceptions of several section directors relating to how the form should be. Think-aloud protocols in individual interviews helped users to become aware of the problems they faced on a daily basis when using the form (Figures 3 & 4). Users normally compensate for design deficiencies without being conscious of it. They might believe that the forms are the way they should be, and that there is no alternative. We worked within a general framework of empathy— empathy for users that faced constant obstacles when filling or transcribing the form.
Surprisingly, the form had been in use for fifteen years before we came to work on it. While it is normally very difficult to get quality time from users such as doctors, particularly in Italy where there is a sense of self-importance in the profession that makes most of them unreachable, we were able to do so. We think this was so partly because they discovered through the think-aloud exercise that there were indeed problems with the form, and partly because they had not been responsible for its development. In other circumstances, when meeting other section directors and asking them about the quality of the forms in their department, every one said they were very good, with some indicating that they themselves had created them.
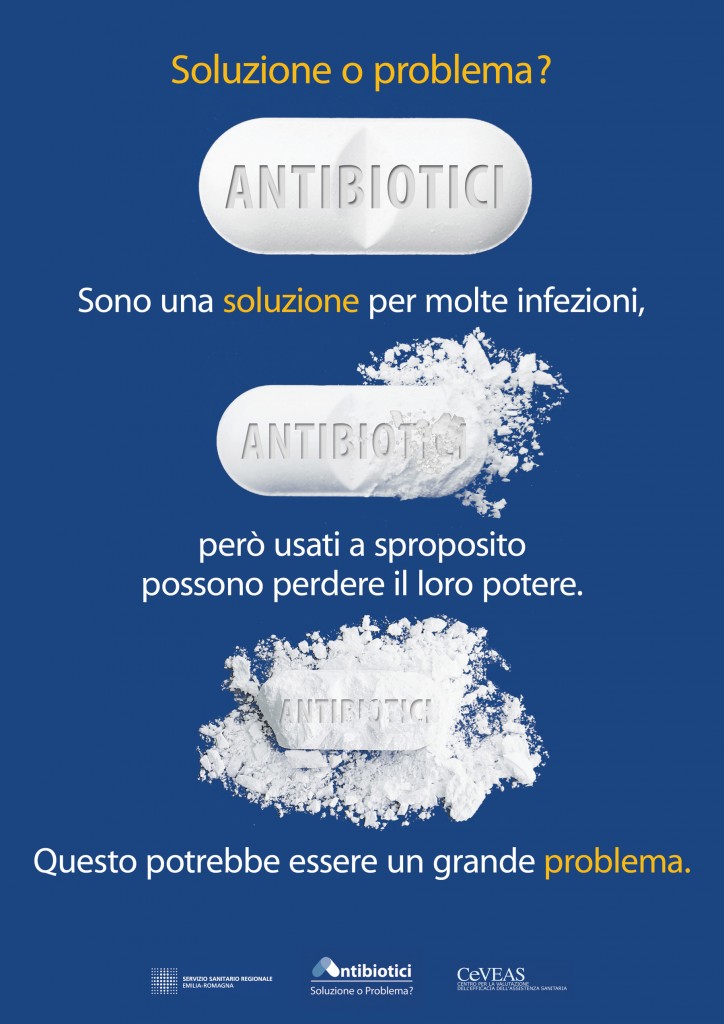
Example Two: Antibiotic Abuse Campaign
 In 2011, we were called to improve the visual details of a brochure aimed at reducing the abuse of antibiotics, a recognized hazard all over Europe. Their call was the beginning of a problem, as a conflict of assumptions emerged: they expected us to realize their ideas, and we expected to be active members in the conception of the campaign including user interviews, prototype evaluations and interdisciplinary work, and at all other stages of the development of the project, including its implementation.
In 2011, we were called to improve the visual details of a brochure aimed at reducing the abuse of antibiotics, a recognized hazard all over Europe. Their call was the beginning of a problem, as a conflict of assumptions emerged: they expected us to realize their ideas, and we expected to be active members in the conception of the campaign including user interviews, prototype evaluations and interdisciplinary work, and at all other stages of the development of the project, including its implementation.
Our client consisted of seven people from different health disciplines – epidemiology, pneumology, clinical pharmacology, infectology, and medicine – in a government agency that evaluates health services in a region of Italy. In addition to the health specialists, there was a person dedicated to crafting the agency’s communications. We somehow inherited an internal conflict over ownership of the project that included defensiveness about each person’s discipline.
One of the members did not want to attack antibiotics, and required the message to be dual: something like “antibiotics are good for this and that, but they can be bad if not used properly.” Although we did not manage to eliminate the positive aspect of the message completely, we were able to reduce its importance to a minimum at the final stage. This compromise was achieved at the final meeting before going to production when we managed to persuade the group using arguments based on evidence about the negative effects of presenting ambiguous messages in health communications.
Instead of adhering to the prototype the client gave us, we made a substantially different and well-argued proposal for the text and visual structure. Our proposed brochure was conceived of as a tool that would facilitate communication between a doctor and patient about when to use antibiotics; it included three scenarios and also room for a doctor’s prescription and indications. It was complemented by two additional pieces: a pocket size brochure, and a poster in two sizes, tabloid and double tabloid (Figure 5). Collaboration on the project happened at different levels: a) the clients proposed a brochure, b) we presented a counter proposal that, in the main, was accepted and c) they provided accurate information for the content of the text and an entry to the family physicians and pharmacists, who were key players in the campaign.
The clients did not want to move forward without all members’ consent. To achieve this, we developed five prototypes of the main image for the project, and evaluated the prototypes with users. This helped the client group to achieve consensus, though they ultimately chose the users’ second choice, as it was, in the clients’ judgment, better. Flexibility and resilience were essential for everybody involved in this project.
It was our conception of design as a collaborative enterprise that allowed the group to move forward and obtain, in the end, a statistically significant reduction in the use of antibiotics. On our own, we could not have achieved the results the campaign obtained. We believe that the client could not have, either. The collaboration was not as comprehensive as it could have been, but given established roles within the culture, it was successful, and all parties were happy with the results. The agency provided us with accurate factual content and their understanding of the local situation around antibiotics use, and identified and worked with the gatekeepers. We provided our communication design expertise using a user-centered, evidence-based and results-oriented approach.
Conclusion: Design as Collective Intelligence
Every design problem is situated, and never exactly repeats the problems one has faced before. Every project involves different people, different purposes, different resources, and different environments that must be understood. However different, every project shares the same goal: the improved welfare of people.
Identifying what information one has to acquire, how to acquire it, and the people one needs to work with are the first steps toward developing a responsible design project. Designing is not only a technical profession: one also requires social skills, awareness of cultural values, and an empathetic framework to design with others in a collectively intelligent way.